Nagehan Ayakta MD, Amir Aminlari MD
Table of Contents
- Knobology
- Physics
- Echo
- IVC
- Aorta
- Lungs
- RUSH exam – rapid ultrasound for shock and hypotension
- Renal
- Gallbladder
- Small Bowel Obstruction (SBO)
- Appendicitis
- Diverticulitis
- Ocular ultrasound
- Soft tissue
- MSK
- DVT
Knobology:
- video
- Every machine has Power, transducers, gain and depth
- Power – total energy delivered by transducer. Normally fixed to avoid adverse biologic effects
- Gain – degree of amplification of the returning signal, similar to volume on radio.
- Probes/transducers
- Phased-array – lowest frequency (1-5Hz) and great for deep structures. i.e. heart
- Curvilinear – middle frequency (2-5 Hz) and great for abdomen, retroperitoneal, OBGYN studies
- Linear – highest frequency (5-15Hz)and best for superficial structures. Great for lung sliding, vascular access, soft tissue and MSK, venous compression studies
- Moving the transducer
- Fanning – pronate-supinate motion
- Rocking – extent-flex motion of your wrist
- Rotating/twisting
Physics:
- Video
- 5 parameters relevant to a pulsed ultrasound:
- Pulse duration
- Pulse repetition period
- Pulse repetition frequency
- Duty factor
- Spatial pulse length
- Pulse duration- length of time from beginning to the end of a pulse
- Pulse repetition period – length of time from beginning of one pulse to the next so includes the pulse duration + listening time
- Pulse repetition frequency (PRF) – number of pulses per second
- Similar to frequency but refers to pulses/sec rather than cycles/sec
- Changed by adjusting the imaging depth – increase in depth, decreases PRF because listening time increases
- Increase in frequency increases resolution but also increases attenuation by increasing scattering
- Duty factor – percentage of time spent producing a pulse
- Affected by
- imaging depth – increasing depth, increases DF
- PRF – increasing PRF, increases DF
- PD – increasing PD, increases DF
- PRP – increasing PRP, decreases DF
- DF (%) = PD(sec) / PRP(sec) * 100
- Affected by
- Spatial pulse length – length or distance of a pulse
(Source: Bedside US volume 1)
- The returning echo intensity of the image is proportional to the grayscale of the pixel of information
- Stronger signal aka more echoes means brighter dot
- Attenuation – loss of energy as the sound waves move through a medium
- Increase in frequency, increases attenuation
- Increase in distance, increases attenuation
(Source: Bedside US volume 1)
- Absorption – conversion of soundwave to heat, leading to attenuation. occurs most with soft tissue
- Reflection – redirection of sound back to probe leads to attenuation
- Scattering – wave reflected in different directions, occurs with media with irregular boundaries such as in lungs. Increase in frequency, increases scattering
- Refraction – redirection of part of sound wave when it crosses from medium to another
- Attenuation coefficient – amount of attenuation per centimeter of tissue, increases with increased frequency.
- Impedance – resistance to the propagation of sound, characteristic of medium and correlated with density and propagation speed
- Relative impedance: bone>>muscle>fat>blood>water>>>>>air
- Angle of incidence or insonation – need to scan perpendicular to object of interest to maximize returning echoes and improve image quality
(Source: Bedside US volume 1)
- Resolution:
- Axial – distinguish between objects in a plane parallel to ultrasound beam, shorter pulses (lower spatial pulse length) leads to better images
- Lateral – distinguish between objects in a plane perpendicular to ultrasound beam aka lying horizontal tissue. Closer array of crystals means better images as well as higher frequency and lower gain
- Temporal resolution aka frame rate – detect position of moving objects in a given time. More frames per second is higher resolution. Decreasing depth is also better
- Scanning modes:
- B-mode – grayscale ultrasound, B=brightness
- M-mode – shows movement of tissue over time
- Vertical axis is depth and corresponds to B-mode image
- Horizontal axis is time
(Source: Bedside US volume 1)
- Color doppler – measures mean velocity and direction of flow, shown over a B-mode image
- Color scale : superior colors represent flow toward the probe and inferior colors away from the probe
- Power doppler – averages flow over several frames, has more sensitivity for eval of low flow states (testicular or ovarian flow) but no info on flow direction
- Spectral doppler – uses continuous or pulsed waves to quantitatively assess flow velocity at a single point. Rate of change of flow. Used with cardiac imaging
(Source: Bedside US volume 1)
- Artifacts:
- video
- Acoustic shadowing – failure of US bream to pass through an object b/c of attenuation or reflection. occurs behind a stone or bone
(Source: Bedside US volume 1)
- Gain artifact – excessive amplification of returning echo leading to invisibility of anechoic structures aka fluid
(Source: Bedside US volume 1)
- Posterior acoustic enhancement – brighter signal behind a liquid structure because of less attenuation
(Source: Bedside US volume 1)
- Reverberation – occurs when two reflectors line parallel to each other and perpendicular to the US wave so that sound gets trapped between the two highly echogenic structures and bounces back and forth like a ping-pong. Ex: A-lines on lungs
(Source: Bedside US volume 1)
- Mirror artifact – image appears on both sides of a strong reflector such as the diaphragm
(Source: Bedside US volume 1)
(Source: Bedside US volume 1)
- Lateral cystic shadowing/edge artifact – occurs when sound waves hit a rounded structure and some of the waves don’t return to the prove causing a shadow along the edge
(Source: Bedside US volume 1)
Echo
- Who to get ECHOs on:
- Chest pain
- Dyspnea
- Unexplained hypotension
- Cardiac arrest
- Trauma
- Syncope
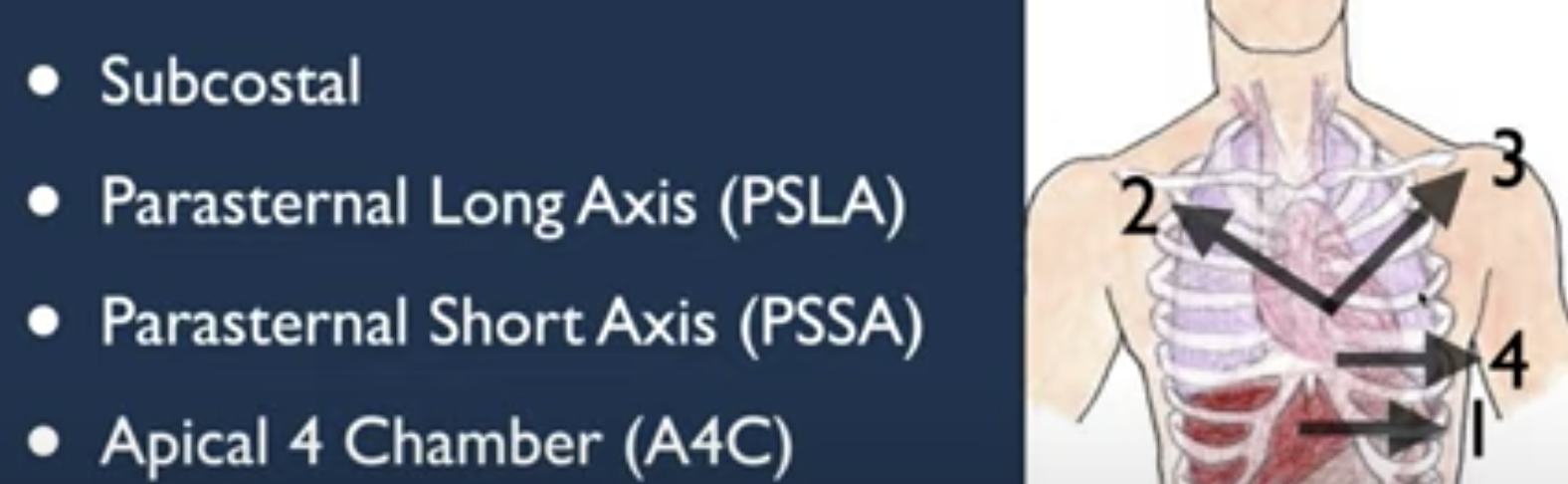
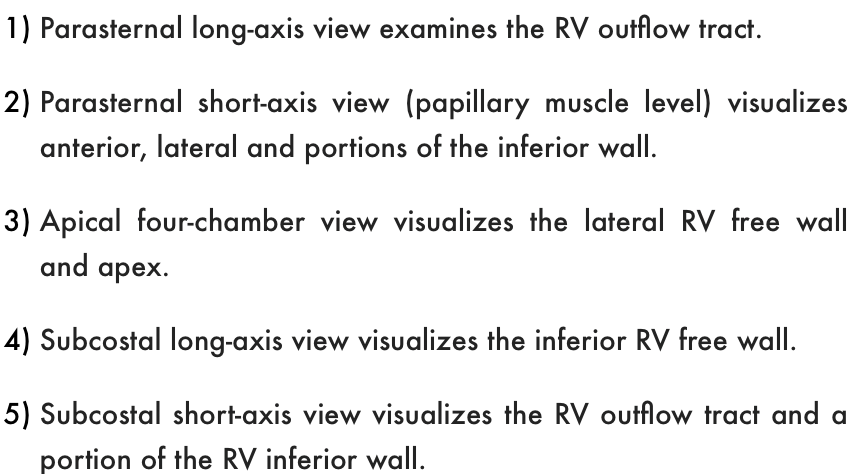
- Window:s
- video
- Subcostal – under the xiphoid, towards L hip
(Source: Bedside US volume 2)
- Parasternal long – ribs 2-5, towards R shoulder (some say L hip)
- Parasternal short – ribs 2-5 towards L shoulder (some say R hip)
- Apical – inferior and lateral to L nipple, towards L hip
- What to look for
- Video
- Chamber sizes – want 1:1:1 for LA, aorta, and RV on parasternal long
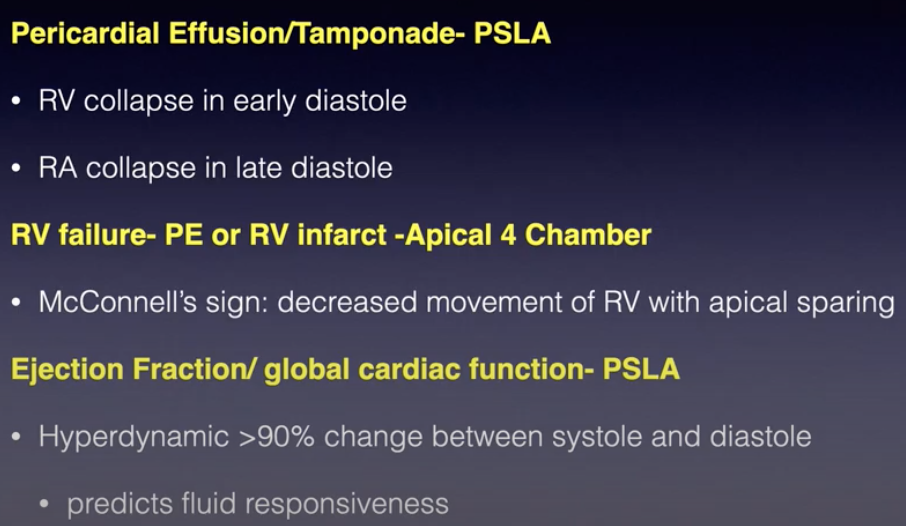
- LV function aka contractility and EF
- Divide into normal (EF>55%), mild-mod depressed (EF 30-55%), severely depressed (EF<30%)
- Quickest way to measure EF is with E-point septal separation (EPSS) which looks at whether MV leaflet touches the septal wall
- Obtain parasternal long axis with adequate view of MV
- Place M-mode through tip of MV
- Identify E and A waves
(Source: Bedside US volume 2)
- E wave – passive filling of LV
- A wave – active filling of LV during atrial contraction
- Measure distance between E wave and the septal wall
(Source: Bedside US volume 2)
- EPSS <0.7cm/hitting the septum is normal EF
- EPSS >1.0cm is reduced EF
- LVEF = 75.5 – (2.5*EPSS)
- EPSS can be misleading with AR or MS
- Can also be hyperdynamic with increased EF – right mitral valve leaflet hits the septum
- This can occur with hypovolemia or vasodilation
- don’t confuse this with tachy with normal EF which wouldn’t have LV collapse like in hyperdynamic
- Calculate CO: =SV*HR
- SV=LVOT area * velocity time integral (VTI)
- LVOT area - measured on parasternal long in mid-systole aka max leaflet separation, (pi*diameter^2) / 4; this stays the same for a patient and does not have to be repeated, normal is 2cm
- VTI - measured on apical long (or 5 chamber view) with pulsed waveform doppler through the LVOT
- Normal 18-22cm
- With afib, measure VTI 5-10 times and average it
(Source: Bedside US volume 2)
(Source: Bedside US volume 2)
- You can calculate fluid responsiveness by doing the passive leg raise in spontaneously breathing patients
- first measure CO with patient sitting at 30-45degrees, then lay them flat and hold their legs up for 2 mins and then recalculate CO (by remeasuring VTI) to see if the CO increases
- Change in SV >10-15% is a sensitive predictor of volume responsiveness
- In mechanically ventilated pts, use SV variation with respiration and degree of IVC collapse to determine fluid responsiveness
- Pericardial effusion
- Video
- Runs anterior or medial to descending thoracic aorta (pleural effusions are posterior or lateral to it)
- Grades
- Small: <0.5cm
- Moderate: 0.5-2.0cm
- Large: >2cm
- Can be focal, organized, loculated or circumferential
- Don’t confuse with epicardial fat pads which are anterior and hypoechoic
- ECHO findings of tamponade:
- video
- RV free wall inversion/collapse during ventricular diastole (hallmark finding)
- RA inversion/collapse during ventricular systole (an earlier finding)
- Increased respiratory variation of mitral or tricuspid inflow velocities above baseline variation b/c septum pushes into LV during inspiration as RV fills so there is less flow through MV (>25% drop) during inspiration (leading to pulsus paradoxus aka reduction in SBP by 10-12 during inspiration) and the reverse happens during expiration so less flow through TV during expiration
- Dilated IVC with decreased respiratory variation (called plethoric IVC)
- Right heart failure
- Video 1 and video 2
- Causes: PE, RV infarction, pHTN, COPD
- Perfusion of RV
- RCA perfuses RV free wall, inferior LV wall and inferior LV septum
- LAD perfuses moderator band
(Source: Bedside US volume 2)
- Views of RV on US
- RV dilation
- RV is ~2/3 size of LV on apical 4-chamber; you can also eyeball that RVOT is ~ in size to aorta and LA on parasternal long
- If RV size is equal to LV size, there is moderate RV dilation
- Best compared at apical 4-chamber view at the level of AV valves in diastole
- Flat septum: occurs with acute pressure overload or volume overload
- detected on parasternal short
- Normally should be concave with respect to LV throughout systole and diastole
- Flattening leads to “D” shaped LV – “D sign”
- With acute systolic overload, D is during diastole and systole
- With volume overload, D is only during diastole
(Source: Bedside US volume 2)
- RV hypertrophy: occurs with chronic pressure overload
- measured on subcostal view during diastole
- Free wall of the RV should measure <5mm
- if it is larger, it is RV hypertrophy which can occur from pHTN, L heart failure, hypertrophic cardiomyopathies or infiltrative cardiomyopathies
- Methods to asses RV systolic function
- Tricuspid annular plane of systolic excursion (TAPSE) method
- RV contracts longitudinally from the Tv to the apex
- the more the TV is displaced during systole, the better the systolic function
- normal movement is 16-20mm on the apical 4-chamber view
- <16mm movement indicated reduced RV systolic function
- Use M-mode – place the indicator over the lateral border of TV annulus and measure distance from diastole to systole
- RV fractional area change (RVFAC) method
- Measure RV area in diastole and systole from apical 4-chamber view
- (End systole-end diastole)/end systole
- The fraction in change should be >40%
- <35% change is abnormal
- Tricuspid annular plane of systolic excursion (TAPSE) method
- McConnell’s sign – finding associated with PE
- Presence of RV mid-wall hypokinesis with normal contraction at the apex
- Low specificity for PE – can occur with pHTN, ARDS, RV MI
- Diastology
- Video
- Diastolic dysfunction defined by poor filling in the ventricles. An early sign is enlarged atria (normal end systole area is <58ml) and poor descent of the base of the atria with each contraction
- Mitral valve inflow –
- Use apical 4 chamber and place pulse wave doppler over tip of the mitral valve when open to see flow into LV
- E wave – early filling, depends on ventricular relaxation and atrial filling pressure. Majority of filling happens during this phase.
- A wave – late filling, depends on ventricular compliance and atrial kick
(Source: Bedside US volume 2)
- Tissue doppler imaging –
- Use apical 4 chamber and place pulse wave doppler over the septum next to the sepal leaflet
- Measures how much the base of the heart (MV, TV, atria) descent with each contraction – more movement the better because shows the ventricles are compliant and not stiff
- E’ – tissue movement with early filling; <8cm/s is diastolic dysfunction
- A’ – tissue movement with atrial kick
- Put the two together
- Impaired relaxation - When the heart can’t relax to allow blood to come in, the E wave is small and the patient is heavily reliant on the atrial kick to get their stroke volume so for these patients, going into AF is detrimental
- Pseudonormal – increased filling pressures from increased preload to overcome the inability of the ventricles to relax so looks normal on mitral flow but the atrial pressure is very high. The tissue movement is also low and more happens with atrial kick
- Restrictive – ventricular pressure is so high that atrial kick has minimal effect at filling the ventricle and there is minimal tissue movement
- Diuresis may help patients with pseudonormal or restrictive diastology
(Source: Bedside US volume 2)
- Filling pressure is great estimate for pulmonary wedge pressure and can be used to guide fluid resuscitation
(Source: Bedside US volume 2)

IVC
- Video
- CVP is a poor predictor of fluid responsiveness!! This is because the relationship between CVP aka filling pressure of RA and stroke volume/cardiac output is NOT linear!
(Source: Bedside US volume 1)
- Fluid responsiveness is the hearts ability to increase CO with increased preload
- Dynamic measurements of IVC and cardiac chambers with US give a better idea of fluid responsiveness
- With spontaneous inspiration, intrathoracic pressure decreases, venous return increases, and stroke volume increases
- With mechanical inspiration, intrathoracic pressure increases, venous return decreases, and SV decreases BUT there is also increased LV preload because of increased pulmonary venous return to the heart so there are cyclical changes in SV with ventilated patients
- Measure IVC 2cm below the RA or 1cm below the hepatic vein
- IVC decreases volume with inspiration typically and need to compare Dmax to Dmin to calculate the collapse percentage
- With 50% change in spontaneous breathing, fluids won’t hurt the patient aka it can tolerate it (not the same as volume responsive)
- In mechanically ventilated patients, IVC distension >18% with passive inspiration predicts fluid responsiveness
- Correlating IVC to CVP
can give fluids for CVP<5
Aorta
- Video
- Indicated for abdominal pain, back pain, chest pain, pulsatile abdominal mass, renal colic, syncope, hypotension, weakness, neurologic changes in the extremities
- Esp >60yo
- Hx of HTN or smoking
- Can visualize the celiac trunk (common hepatic and spleen usually), SMA and maybe renal arteries – hard to see gonadal or IMA
- Aorta bifurcates at the level of the umbilicus
- Troubleshooting:
- Press deeply to get through the bowel gas!
- Fan through to move the bowel gas
- Lay patient completely flat with hips and knees flexed to relax their abdominal muscles
- Campbells’ view – right mid-axillary line
- Aortic diameter should be <3cm with tapering distally – measure the aorta 3 times in the transverse plane outer wall to outer wall!
- Most AAA are infrarenal!
- Side note for thoracic aorta: Don’t measure right at the root! b/c it can be dilated at the root without an aneurysm
(Source: 5minsono)
- If >5cm, need emergent surgery!
- Also concerning if growth >0.6-0.8cm/yr
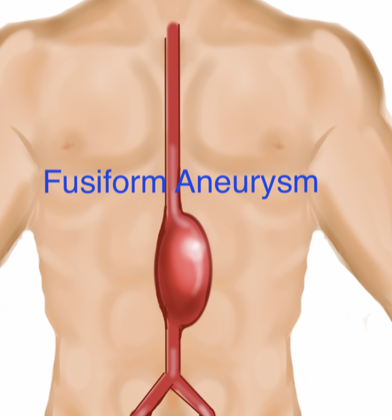
- Types of aneurysms: fusiform is more common
- Fusiform – 90%
(Source: Bedside US volume 1)
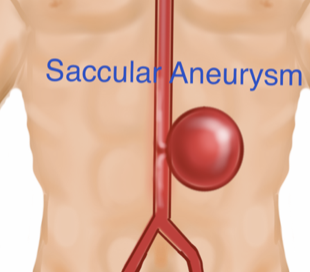
- Saccular – 10%
(Source: Bedside US volume 1)
- Fusiform – 90%
- Aortic dissection
- Video
- Abdominal:
(Source: Bedside US volume 1)
- Indirect signs of thoracic dissection: dilation, regurgitation, effusion
- Don’t forget to the suprasternal view with probe on an angle
normal (Source: 5minsono)
dissection (Source: 5minsono)
- To see thrombi, make sure the gain is low so that the lumen is completely black and the clot will be gray
(Source: Bedside US volume 1)
Lungs
- Ultrasound has good specificity but worse sensitivity for causes of acute dyspnea
- Scans the lungs with 8 zones
(Source: Bedside US volume 1)
- A-lines – “air lines” horizontal reverberation artifact that occurs with normal lungs because the beams reflect back and forth between the skin and the pleura creating equally spaced horizontal lines
- B-lines – vertical lines that occur with increased density in the lung - interstitial thickening (fluid or fibrosis) or alveolar fluid aka helps detect pulmonary edema, pulmonary fibrosis, and infection
- video
- Pulm edema will have thin pleural lines in addition to B lines
- Infection/inflammation will cause irregular pleural lines
(Source: Bedside US volume 1)
- B lines are
- Are at least 18cm deep
- Moves with respiration as the pleural line moves
- Thin, single vertical lines but becomes wedge-shaped with increasing interstitial fluid
- More B lines = worse prognosis
- B lines resolve within hours of diuresis!!
(Source: Bedside US volume 1)
(Source: 5minsono)
- Focal B-lines in the setting of chest trauma, think pulmonary contusion
- Pneumothorax – look for lung sliding with “ants on a log” or M mode to look for movement “seashore sign”
- Video
- barcode at the top where tissue doesn’t move and then sand like/seashore appearance where the lung moves
(Source: Bedside US volume 1)
- You see barcode sign on M mode with PTX b/c of reverberation artifact
(Source: Bedside US volume 1)
- False positives: Lack of lung sliding can also occur with scarring of pleura, pneumonia with adhesions – to differentiate these diagnoses from PTX, look for the comet-tail which is a vertical bright line that forms from reverberation artifact of the visceral and parietal pleura touching each other
- Scanning only the anterior chest may miss apical PTX – scan superiorly or supraclavicularly to find apical PTX
- Lung point – where the visceral pleura reattaches to the chest wall, pathognomonic for PTX
- Pleural effusions
- Video1 and video2
- 2 ways to identify pleural effusions on RUQ and LUQ:
- Lack of mirror image artifact
- Spine sign
- Diaphragm can cause a mirror image artifact when there is no fluid in the lungs
(Source: Bedside US volume 1)
- reflection of the liver above the diaphragm – indicates an aerated lung!
- No reflection means pleural effusion:
(Source: Bedside US volume 1)
- Spine sign:
- Normally the spine cannot be seen underneath the lungs because air in the lungs scatter the sound beams
- Being able to see the spine above the diaphragm means there is fluid in the lungs that allows for sound to travel
(Source: Bedside US volume 1)
- Can detect pleural effusions on the left side with parasternal long axis – fluid posterior and inferior to the descending aorta
- Can detect pleural effusions on the right with subxiphoid view
(Source: Bedside US volume 1)
- Lung hepatization – fluid in the alveoli transmit sound better than air and make lungs look like a solid organ
- Well correlated with consolidation on CXR and CT chest
- Can follow progression of disease from focal areas of B lines to coalescence of B lines and irregular pleural lines to consolidation
(Source: Bedside US volume 1)
- Can even distinguish consolidation from atelectasis by looking at bronchi (hyperechoic columns) which move with consolidation as air continues to flow through them but are not mobile with atelectasis
- Pneumonia:
- video
- Look for air bronchograms, B-lines, pleural effusions, subpleural consolidation, and fluid bronchograms
- Static air bronchograms are the hyperechoic areas:
(Source: Bedside US volume 1)
- Dynamic air bronchogram moves with respiration
(Source: 5minsono)
- Spine sign:
(Source: 5minsono)
- Viral pneumonia- video
- Scan across the chest and the back! The most important place is not miss are the lower lobes
- Can use curvilinear and scan across while looking at the pleural space
(Source: 5minsono)
RUSH exam
- video
- Used for undifferentiated hypotension
- Includes HI-MAP:
- Heart
- IVC
- Morison’s Pouch aka FAST
- Aorta
- Pneumothorax (PTX)
(Source: Bedside US volume 1)
- Heart - use parasternal long and apical to look for pericardial effusion/tamponade, RV failure for PE, and LV function
- IVC - use sagittal axis with curvilinear to look for diameter and collapse to estimate volume response
- Morison’s aka FAST – look for intraabdominal fluid
- video
- Can detect >200-300cc
- 0.5cm stripe in Morison’s is about 500cc fluid; 1.0 cm is 1000cc
- Most important area to look at in RUQ is the caudal tip of liver and the inferior pole of kidney
- Most important area to look at in the LUQ is between spleen and diaphragm because fluid can accumulate anywhere around the spleen
- Aorta – look at size of aorta (normal <3cm, if >5cm and shock, assume ruptured AAA until proven otherwise) at subxiphoid, suprarenal, intrarenal, and at bifurcation for AAA and dissection
- Pleura – for PTX, effusions, CHF, consolidation, esp look for PTX after central line, pacemaker placement, lung biopsy, or thoracentesis
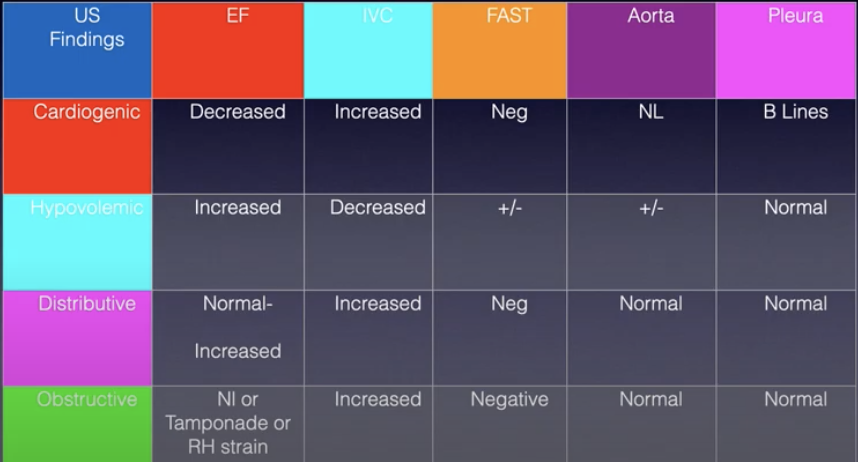
- Differentiating shock states:
Renal
- Video
- Use US over CT when renal pathology is high and other etiologies of flank pain are low
- Stones are seen well when in the kidney but not after they pass into the ureter – but can diagnose based on secondary findings like hydronephrosis
(Source: Bedside US volume 1)
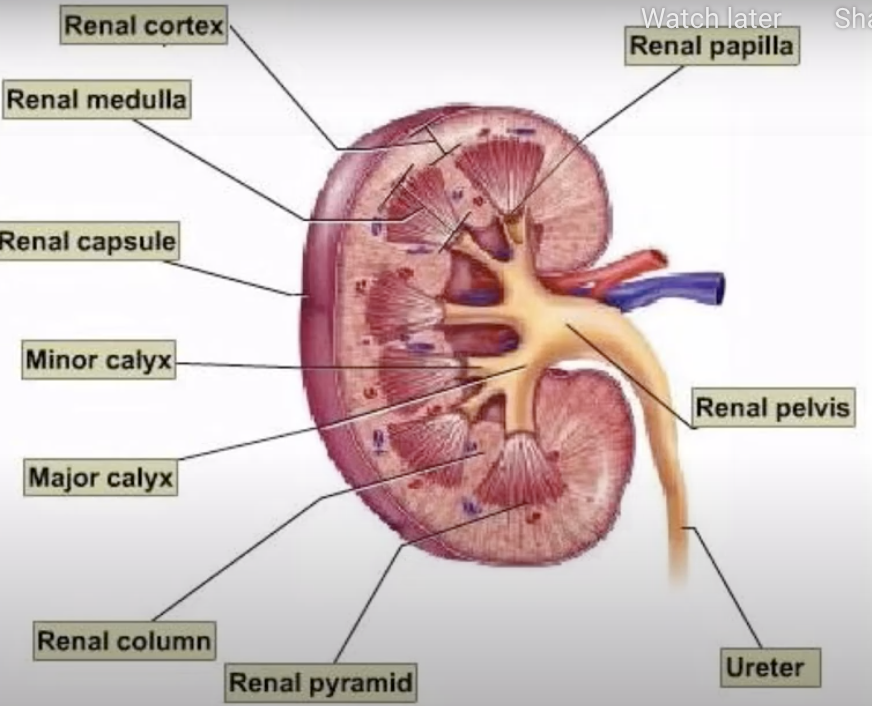
- Normal kidney on US:
- Renal cortex is hypoechoic to the liver/spleen but hyperechoic compared to the medulla which has the pyramids but are not visible in normal kidney
- Pelvis is more hyperechoic
(Source: Bedside US volume 1)
- 9-12 cm long and 4-5cm wide; no more than 2cm variation between the R and L
- Cortex is typically 1-2cm thick – thinner may mean hydro; thicker may mean pyelo
- You can give a fluid bolus prior to scanning to improve sensitivity for hydronephrosis in patients who may be hypovolemic
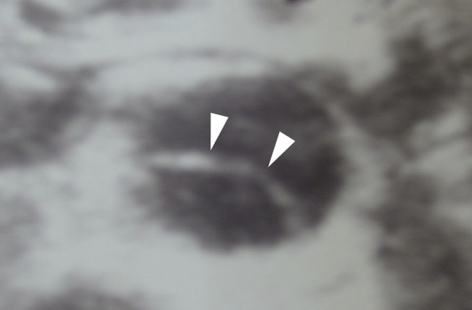
- Hydronephrosis grading:
- Mild – enlargement of calices with preservation of renal papillae/pyramids
- Moderate – blunting of calices with obliteration of papillae
- Severe – cortical thinning
(Source: Bedside US volume 1)
- Grading is associated with stone size
- Small stones <5mm pass spontaneously
- Large stones >10mm need surgery
- Always check the aorta!
(Source: Bedside US volume 1)
- US helps diagnose nephrolithiasis in low and mod STONE score patients but not as helpful for patients with high STONE scores – STONE Plus study
- Hydro does not equal stone! Other diagnoses can cause hydro such as pyelo, appendicitis, prostate pathology, uterine cancers etc.
- Bladder volume measure: L*H*W*0.75 (video)

Gallbladder
- Video
- Use curvilinear probe and look right below the costal margin in transverse and sagittal views
- Troubleshoot: turn the patient to left lateral decubitus or ask them to take a deep breath and hold
- Findings: gallstones, gallbladder wall thickening, pericholecystic fluid and CBD dilation
- If you identify a stone, move the patient to make sure the stone moves, otherwise it may be an impacted stone or a mass
- Measure CBD as medially as possible and use color to make sure it isn’t the hepatic artery
- Identify the portal triad which the neck of the GB points to
- Mickey mouse sign is the portal triad
(Source: Bedside US volume 1)
(Source: Bedside US volume 1)
- the large vessel below both is the portal vein – CBD is anterior to PV
(Source: Bedside US volume 1)
- Sizes:
- GB length is 7-8cm and width is 2-3cm
- GB wall thickness is <0.3cm
- CBD <0.6cm; add 0.1cm for every decade of life after 60
- Cholecystitis diagnosis:
- Gallstone presence
- GB wall thickness >0.3cm
- Pericholecystic fluid
- Sonographic murphy’s sign
- Wall Echo Sign (WES)- gallbladder filled with stones and contracted so only thing seen is an echogenic line near the anterior wall of the GB
(Source: Bedside US volume 2)
- Choledocholithiasis diagnosis:
- CBD >0.7cm (>1.0cm in a patient with a cholecystectomy)
- Dilated gallbladder
- Gallstones
Small Bowel Obstruction (SBO)
- Video
- US is more sensitive than abdominal XR
- Use curvilinear probe – highest frequency
- Graded compressions is used to evaluate bowels
- Start at RLQ in transverse and push down every 2-3cm as you work towards the LLQ
- Then do longitudinal starting in LLW and move up and down until you get to the RLQ
(Source: Bedside US volume 2)
- If you find dilated bowel, follow until the transition point to diagnose an obstruction vs ileus
- Findings:
- Fluid filled loops of bowel
- Small bowel >2.5-3cm, non-compressible
- Back and forth peristalsis – means there is an obstruction distal to it
- No movement at all
- Wall edema – wall thickness >4mm
- Free fluid in the abdomen – Tanga sign is a triangular shape of free fluid around dilated bowel
- If ruptured, can see pneumoperitoneum
- Video
- Use linear probe
- Look at the most anterior aspect of abdomen while lying flat. Can try left lateral decubitus but patient may be too unstable for this
- Look for Enhanced Peritoneal Stripe Sign (EPSS)
- The peritoneum is bright linear tissue right underneath the subQ tissue
- When there is air in the abdomen, the peritoneal strip looks even brighter. Circle below shows the transitional from normal peritoneum on the left to the enhanced air represented free air on the right
(Source: 5minsono)
- 0.2mL of air has good sensitivity and specificity – better than XR but CT is still the gold standard
Appendicitis
- Video
- US is specific but not sensitive for appendicitis
- Use linear or curvilinear probe (if depth needed in obese patients)
- Ask the patient where it hurts and put the probe right on it!
- Troubleshoot: ask right leg over left leg to bring appendicitis closer to abdominal wall
- Go between iliac crest (lateral), iliac artery (medial), and psoas muscle (inferior):
- appendicitis will be on top of iliac artery so go up and down on the artery until you see it
- compress down to the psoas to make sure it isn’t compressible
- Findings:
- Diameter >6mm
- Non-compressible
- “ring of fire” – increased blood flow around the appendix
- Edema around the edema
- Fecalith
(Source: Bedside US volume 2)
Diverticulitis
- Video
- Can use any of the transducers but curvilinear the best
- Start in the LLQ and do graded compression
- Findings:
- Diverticula – out-pouching of the abdominal wall (arrow)
(Source: 5minsono)
- Bowel wall >5mm.
(Source: 5minsono)
- Prominent fluid filled loops of bowel
- Pericolic fluid collections – usually around the loops of bowel rather than at the FAST views
- increased pericolic fat (hyperechoic)
- intraabdominal abscesses
(Source: 5minsono)
- Diverticula – out-pouching of the abdominal wall (arrow)
Ocular ultrasound
- Use linear high frequency probe
- lots of gel to avoid pressure on the eye
- can use tegaderm if patient can’t close their eye completely
- Low gain to see the optic nerve
- Higher gain to look for retinal detachment
- Can help diagnose:
- Retinal detachment
- Hemorrhage
- Lens dislocation
- Elevated ICP
- Globe rupture
- Normal eye on US
(Source: Bedside US volume 2)
- Globe rupture:
- Don’t do US if it is an obvious rupture!
- Findings: decreased size of the globe, anterior chamber collapse, buckling of the sclera
(Source: Bedside US volume 2)
- Foreign body:
- Glass and some metals can be missed on CT so US can be helpful
- Findings: hyperechoic structure with shadowing or reverberation artifact
(Source: Bedside US volume 2)
- Retinal detachment:
- Video
- US has 97% sensitivity and 92% specificity
- Findings: serpentine echogenic structure attached to the optic nerve at the posterior wall of globe
- It remains fixed to the posterior wall which helps distinguish it from vitreous hemorrhage or detachment
(Source: Bedside US volume 2)
- Complete retinal detachment: V-shape within the globe
(Source: Bedside US volume 2)
- Identify the macula by going directly back and perpendicular to the middle of the lens – if macula is attached, can save vision and ophtho consult is emergent!
- It remains fixed to the posterior wall which helps distinguish it from vitreous hemorrhage or detachment
- Vitreous hemorrhage/posterior detachment findings:
- globular hyperechoic structure
- subtle hemorrhage may only be seen with higher gain
(Source: 5minsono)
- Lens dislocation findings: posterior displaced lens
(Source: Bedside US volume 2)
- ICP Findings: Dilation of optic nerve
- Video
- Measure 3cm back from the retina when the sides are parallel
- Normal nerve width is <5mm – outer to outer wall
(Source: Bedside US volume 2)
- >5mm has 90% sensitivity and 85% specificity for ICP >20mmHg
(Source: Bedside US volume 2)
- Retrobulbar hematoma
- Retrobulbar area is the area of acoustic enhancement posterior to the globe
- Findings: hypoechoic structure within the retrobulbar area
(Source: Bedside US volume 2)
- Central retinal artery occlusion
- Video
- Look for the retrobulbar spot sign – hyperechoic area in the optic nerve (arrow) which represents the actual thrombus
(Source: 5minsono)
- This is only seen in white thrombus which is embolic cholesterol and fibrin. Don’t have this sign in red thrombi which is thromboembolic
- Compare this to optic nerve drusen (on the right below) which is more benign and located at the very distal end of the optic nerve and is bigger compared to CRAO which is seen a little more proximally and smaller
(Source: 5minsono)
Soft tissue
- video
- Use linear probe with lots of gel
- If too painful, can use a water bath to image the affected area
- Normal tissue:
(Source: Bedside US volume 2)
- Cellulitis findings:
- Distortion of the normal architecture – early in the course or mild
(Source: 5minsono)
- Cobblestoning – late in the disease course or severe
(Source: 5minsono)
- Distortion of the normal architecture – early in the course or mild
- Abscess: irregular but defined border, large hypoechoic or heterogenous echogenicity
(Source: 5minsono)
- With pressure, you can see the movement of pus – pus peristalsis
- Make sure there isn’t vasculature or nerves within the abscess!
- Abscess mimics: inflamed lymph nodes, malignant mass, abdominal wall hernia, post-procedural hematoma
- Necrotizing fasciitis – air within the soft tissue (green below) and 4mm of fluid overlying the deep fascial layer
- Video
(Source: 5minsono)
- SEFE exam describes criteria of nec fasc - subQ thickening, subQ air, perifascial fluid, abnormal muscle architecture
- All foreign bodies – radiolucent or opaque – show up as hyperechoic on US
- Video
- Can see glass, wood, metal
- Findings: object itself, posterior enhancement, tissue edema, granulation tissue around it (presents as halo sign – hypoechoic halo surrounding hyperechoic FB – within 24hours)
(Source: 5minsono)
MSK
- Video
- Use linear frequency but can use curvilinear for deeper structures
- Important concept in MSK – anisotropy – structures look different at different angles of insonation
- Hyperechoic when perpendicular to the nerve, tendon, and lesser extent muscle
- Hypoechoic when probe is not 90degrees to the structure
(Source: Bedside US volume 2)
- This can be lost with pathology such as a tear or inflammation
- Views to get: two orthogonal planes, contralateral examination, dynamic examination, and application of probe pressure.
- Nerves – hyperechoic with honey-combing pattern
(Source: Bedside US volume 2)
- Muscle
normal (Source: Bedside US volume 2)
- Grade 1muscle injury– muscle sheath and fascia intact with swelling and enlargement of muscle body present, can see intramuscular hematoma
(Source: Bedside US volume 2)
- Grade 2 – muscle sheath and fascia torn so you see blood traveling between muscle groups
(Source: Bedside US volume 2)
- Grade 3 – complete rupture of muscle body – swollen, retracted muscle with hemorrhage
(Source: Bedside US volume 2)
- Calcification occurs as hematoma heals – central calcification first if sarcoma, peripheral first trauma related hematoma
- Myositis – loss of muscular echotexture, hyperechoic muscle fibers, enlarged muscle body, inflammatory/exudative fluid around the muscle
(Source: Bedside US volume 2)
- Grade 1muscle injury– muscle sheath and fascia intact with swelling and enlargement of muscle body present, can see intramuscular hematoma
- Tendons – more uniform hyperechoic brush-like appearance compared to muscle
(Source: Bedside US volume 2)
- Need dynamic imaging to look at integrity of the tendon
- Partial tendon rupture – hypoechoic fluid within the tendon that is not anisotropic or fluid around the tendon/between fascial layers
- Complete tendon rupture – two separate tendon fragments with hemorrhage and retraction
(Source: Bedside US volume 2)
- Ligaments – similar appearance to tendons
- Findings with sprains, rupture, avulsion: enlarged, hemorrhage, loss of anisotropy
- With avulsions, you can also see a bony fragment at the end of a retracted ligament
(Source: Bedside US volume 2)
- Bone and joint spaces
- Good for occult fractures and rib fractures, during fracture reduction, and for joint effusions
- Not as good for fractures of hands, feet, and pelvis
- Findings of fractures:
- discontinuity on the surface of bone with or without a step-off deformity
- angular deformity of bone cortex
- subperiosteal hematoma
(Source: Bedside US volume 2)
- Findings of effusions:
- >7mm effusion is abnormal or if >1mm difference between affected and unaffected side
- Mechanical/inflammatory fluid appears anechoic
(Source: Bedside US volume 2)
- Bloody effusions appear hyperechoic
(Source: Bedside US volume 2)
- Can use US before and after dislocation
(Source: Bedside US volume 2)
DVT
- Video
- Use linear probe – don’t have to do color or doppler for a complete exam
- Assess with 2-point compression technique – femoral and popliteal veins
- Have patient in 20-30degree reverse Trendelenburg position
- External rotation of hip and knee flexed
- Must go 5cm distal to common femoral vein; must evaluate the superficial portions of anterior, posterior and tibial veins coming off of popliteal vein
- Femoral vein is medial to femoral artery
- Popliteal vein is superficial to popliteal artery at the back of the knee
- Findings: A vein must be fully compressible to rule out DVT
References
- 1. Avila, J. (2018). 5 min sono. Core Ultrasound. https://www.coreultrasound.com/5ms/
- 2. Schoenfeld, E. (2013). Introduction to Bedside Ultrasound, Volumes 1 and 2. Society for Academic Emergency Medicine.