
Background
The chief complaint of “dyspnea” represents a very large cohort of patient who present to the emergency department. While acute heart failure (AHF) is a very common diagnosis in the setting of dyspnea, the diagnosis remains challenging when the emergency physician is presented with the undifferentiated dyspneic patient. Interestingly, emergency physicians have varied approaches to the work up and diagnosis of these patients and it is not clear as to which diagnostic element is most crucial in confirming the diagnosis of AHF. Spoiler: Ultrasound proves to be quite useful.
Diagnosing Acute Heart Failure in the Emergency Department: A Systematic Review and Meta-analysis
Clinical Question
What are the operating characteristics of the diagnostic elements available to the emergency physician for diagnosing acute heart failure?
Methods & Study Design
- Design
- This is a systematic review evaluating index test operating characteristics in diagnosing AHF. A medical literature search was performed using PubMed and EMBASE, evaluating peer-reviewed published papers from 1965 through 2015
- Individual systematic reviews for each index test were conducted by two separate physicians and thereafter reconciled to obtain a comprehensive set of studies on the topic. These were then screened against the inclusion/exclusion criteria for final inclusion into the meta-analysis
- The reference standard used was a final diagnosis of AHF based on review of clinical data by independent reviewers who were blinded to the study’s primary index test
- Population
- All studies included involved patients presenting to the emergency department (ED) with the chief complaint of “dyspnea.”
- Outcomes
- Pooled sensitivities, specificities and likelihood ratios (LRs) of index tests for diagnosing acute heart failure in patients presenting to the ED with dyspnea
- They specifically looked at the following index tests in evaluation of AHF: history and physical exam, ECG, chest x-ray, BNP and NT-ProBNP, lung ultrasound (US), and bedside echocardiography
- Excluded
- Patients presenting to urgent care with dyspnea
- Patients with chronic, compensated heart failure
- Studies focusing on prognosis or therapeutics and not the diagnosis of AHF
- Studies with ultrasound images that were not obtained and interpreted by emergency physicians
Results
-
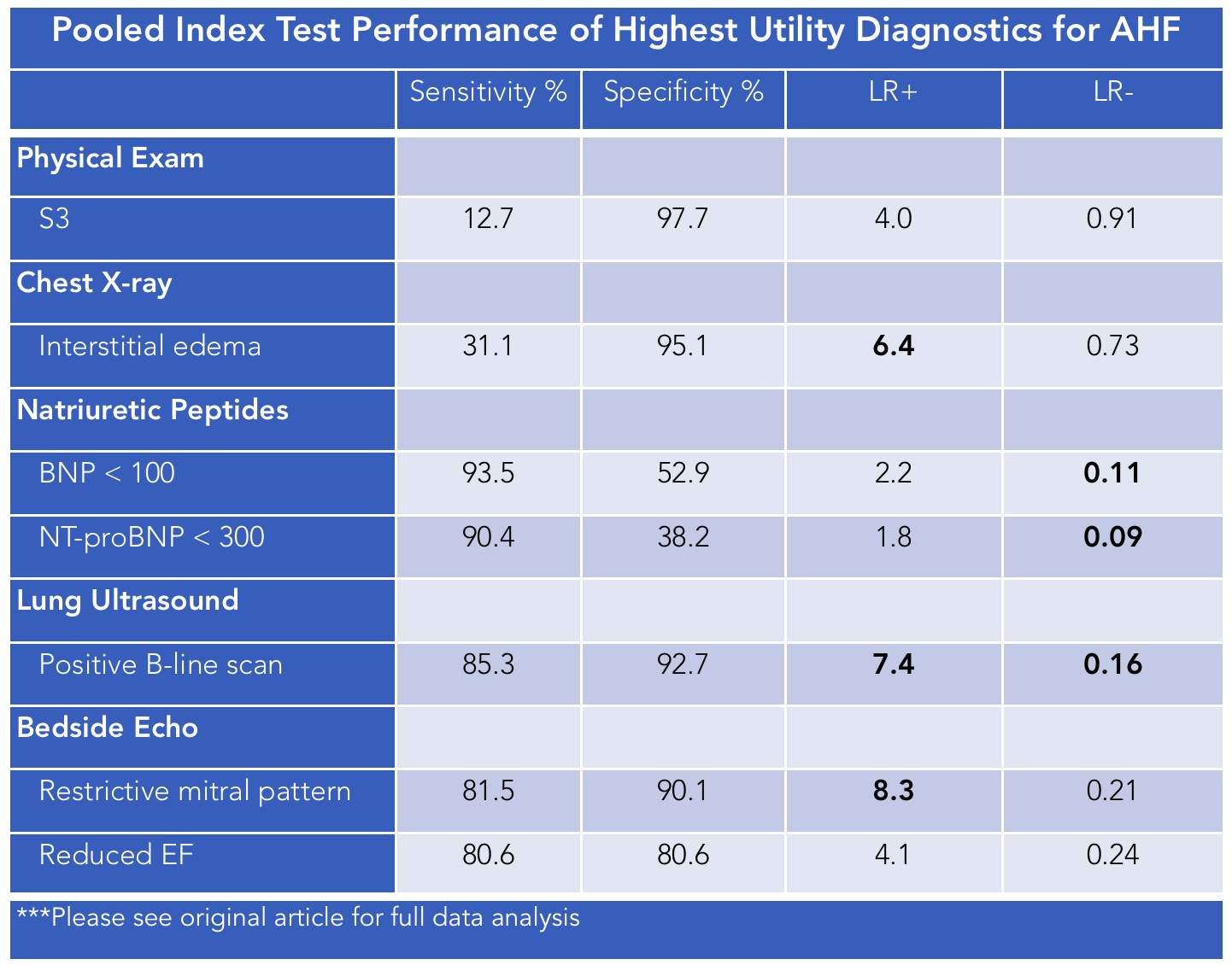
- History and Physical: S3 most specific finding for AHF (+LR 4)
- ECG: Found to be insensitive and unspecific for diagnosing or ruling out AHF
- CXR: Pulmonary edema was the most specific finding (LR + 4.8). All other imaging findings were insensitive for ruling out heart failure
- BNP and NT-Pro-BNP: Quite sensitive for ruling out AHF at a threshold of 100/300pg/dL
- Lung Ultrasound:
- Presence of >3 B-lines in >2 lung fields is very specific for the presence of AHF
- Lack of this also sensitive for ruling out acute heart failure
- High inter-rater reliability
- Bedside Echo
- ED provider evaluation of systolic function had high inter-rater reliability with the ultimate ejection fraction assessed by cardiologists on formal echo
- Restricted Mitral Inflow very specific for ruling in diastolic AHF in patients with preserved systolic function
Strengths & Limitations
- Strengths
- Very thorough analysis of the operating characteristics of a plethora of diagnostic elements and sub-elements available to the emergency physician in diagnosing AHF
- Authors didn’t exclude comorbidities, etiology of AHF or if there was an underlying arrhythmia which increased the generalizability of their results
- All data was screened and evaluated by two separate physicians
- Limitations
- The reference standard was a final diagnosis of AHF made by physicians in retrospective fashion which weakens this as a “gold standard.”
- The authors did not specifically evaluate or reconcile whether the heart failure was left or right sided
- Each of the tests or test characteristics were assessed in isolation to determine the likelihood of heart failure. The likelihood of AHF when considering multiple index tests was not assessed
- As in all large meta-analyses, some spectrum bias may exist as inclusion/exclusion criteria varied among included studies. However, ome of this heterogeneity is likely countered by the pooled analysis and is unlikely to drastically change the calculated LRs
Author's Conclusions
"Bedside lung US and echocardiography appear to the most useful tests for affirming the presence of AHF while natriuretic peptides are valuable in excluding the diagnosis."
Our Conclusions
This is one of the most thorough studies available to assess the likelihood that a patient presenting to the emergency department has acute heart failure based on an index test. There are many old standby diagnostic modalities available to emergency physicians including the history, physical exam, and chest x-ray. Unfortunately, these diagnostic elements are relatively non-specific in establishing that a patient’s acute symptoms are likely or unlikely due to heart failure. BNP and NT Pro BNP are quite useful in ruling out heart failure however these tests take time to result. Ultrasound is rapidly becoming a fundamental tool in every emergency physicians tool belt and should be utilized alongside the primary patient assessment in determining the likelihood that a patient has heart failure. The presence or absence of B lines (>3 in at least 2 fields) is quite specific for ruling in heart failure and the absence is nearly as sensitive as a normal BNP or NT Pro BNP, too. And in the event of systolic heart failure, echo is a great modality to rapidly assess a patient’s pump function; our interpretation is consistent with the formal result obtained by cardiologists [2].
Caution must nevertheless be maintained when evaluating these results. The LRs found in these studies were calculated independently of other findings and in reality, the emergency physician takes multiple factors from the history, physical exam, and other diagnostic modalities, to ultimately come to a definitive diagnosis. Essentially, the short answer is that no single test should be taken as definitive in diagnosis of AHF (or any diagnosis for that matter) and the emergency physician should follow a bayesian approach using pre- and post- test probabilities from their fund of knowledge to rule in and rule out cannot miss diagnoses. Lastly, with regards to this study, physicians should be wary about interpreting these results in the context of renal failure primarily but also superimposed pneumonia or underlying concern for pulmonary embolism as these patients were excluded in a number of papers included in this meta-analysis.
The Bottom Line
Bedside ultrasound to evaluate for the presence or absence of pulmonary edema should be an integral part of the emergency physicians approach to evaluating patients to the emergency department with undifferentiated dyspnea.
Authors
This post was written by Matt Correia, MD PGY-2 at UCSD. It was edited by Michael Macias, MD.
References
-
- Martindale JL, e. (2017). Diagnosing Acute Heart Failure in the Emergency Department: A Systematic Review and Meta-analysis. - PubMed - NCBI . Ncbi.nlm.nih.gov. Retrieved 14 August 2017, from https://www.ncbi.nlm.nih.gov/pubmed/26910112
- Moore CL, e. (2017). Determination of left ventricular function by emergency physician echocardiography of hypotensive patients. - PubMed - NCBI . Ncbi.nlm.nih.gov. Retrieved 14 August 2017, from https://www.ncbi.nlm.nih.gov/pubmed/11874773