
Background
Trauma is the leading cause of death in those younger than 45 years in the United States. Around 80% of injuries are due to blunt trauma with 20% involving penetrating trauma. It is blunt trauma, however, that carries substantial diagnostic challenges due to complex injury patterns and difficult management strategies. This paper sets out to review and summarize the comparisons of different techniques in diagnosis of intra-abdominal injury via physical exam findings, laboratory values, and imaging including bedside ultrasound.
Does This Adult Patient Have a Blunt Intra-abdominal Injury?
Clinical Question
How accurate and reliable are existing symptoms, signs, laboratory tests and bedside imaging studies at diagnosing intra-abdominal injury following blunt abdominal trauma?
Methods & Study Design
- Population
- The study analyzed 12 papers that assessed clinical examination and 22 papers to assess role of FAST in identifying intra-abdominal injury. Sample sizes ranged from 117 to 3435 patients. All studies defined inclusion criteria as adult patients with any blunt abdominal trauma except for 2 studies that included only adult patients in motor vehicle collisions.
- Intervention
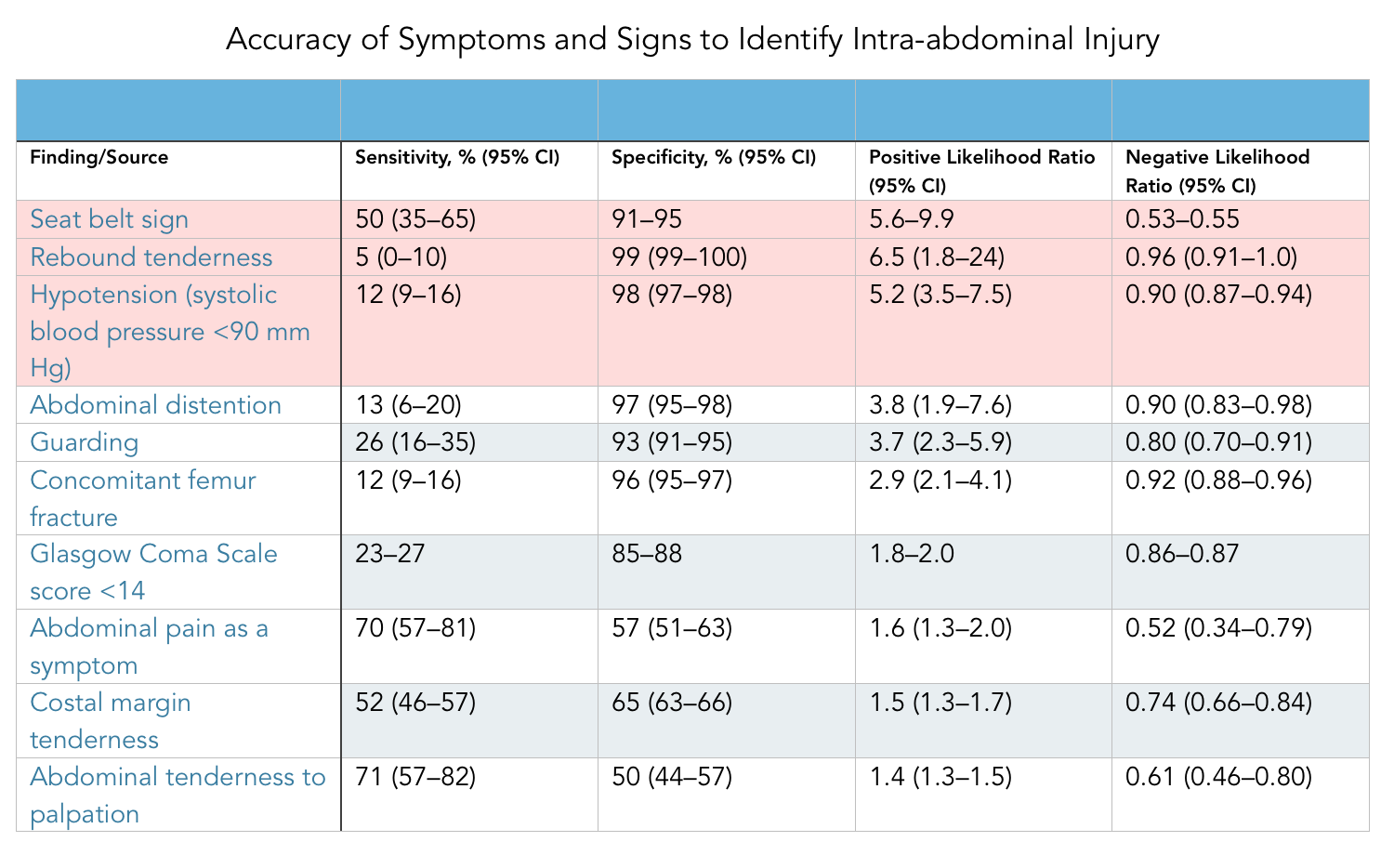
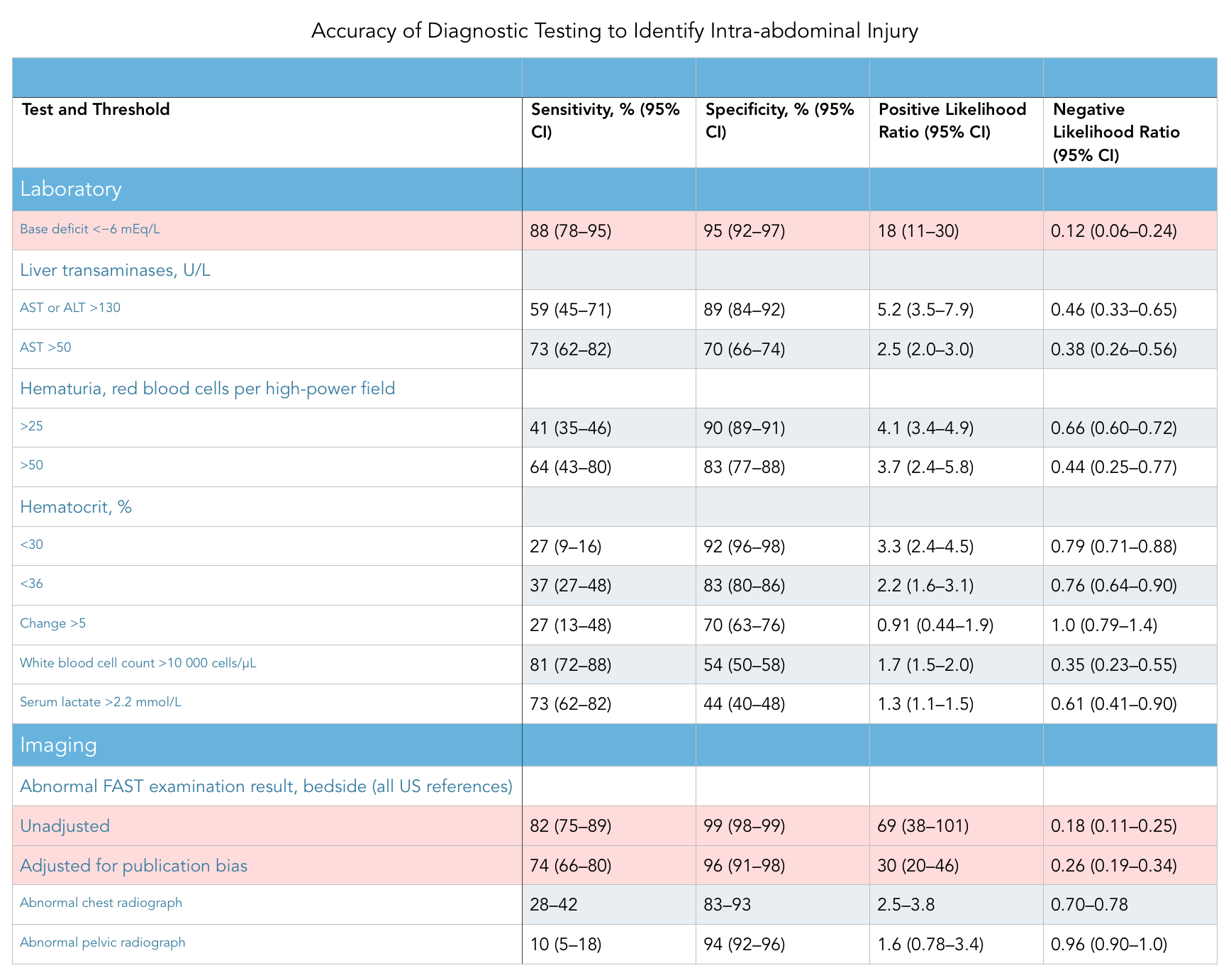
- This particular paper focused on the likelihood ratios of various approaches in predicting intra-abdominal injury including: physical exam findings (i.e rebound tenderness, abdominal distention, guarding, seat belt sign, and hypotension), laboratory tests (i.e. base deficit, hematuria, elevated transaminases and anemia), and FAST examination.
- Outcomes
- Researchers measured specificity, sensitivity, positive likelihood and negative likelihood of the various physical exam, laboratory, and imaging findings associated with blunt trauma.
- Design
- This is a meta-analysis of numerous prospective studies looking at blunt abdominal trauma.
- Excluded
- The publishers chose to include studies that were prospective, with consecutive enrollment and blinding, and included a reference standard (i.e. abdominal CT, DPL, laparotomy, autopsy, or clinical course to detect intra-abdominal injury or hemoperitoneum).
Results
Strengths & Limitations
- Strengths
- Analyzed the biggest publications from top-trauma centers focusing on strength of statistical analysis.
- Created subcategories of studies that focused on FAST in order to ascertain if any of the information was skewed.
- Limitations
- This is a 2012 study that only focused on papers older than 2007, excluding any new techniques and standards as well as imaging advancements of the last decade.
- They did not review studies for clinical outcome, so cannot draw conclusions regarding how change in bedside exam and procedures impact patient care post diagnosis.
- As with all large meta-analysis studies there is always risk of significant heterogeneity from varying study inclusion/exclusion criteria making generalizability complex.
Author's Conclusions
“Bedside ultrasonography has the highest accuracy of all individual findings, but a normal result does not rule out an intra-abdominal injury. Combinations of clinical findings may be most useful to determine which patients do not require further evaluation, but the ideal combination of variables for identifying patients without intra-abdominal injury requires further study.”
Our Conclusions
Overall, this paper reinforces the strength of bedside ultrasonography (adjusted positive LR of 30) as a diagnostic tool of intra-abdominal injury following blunt trauma compared to physical exam and laboratory findings. This reinforces ultrasounds role as the best tool to "rule-in" an intra-abdominal injury. However, it also elucidates a relatively poor sensitivity of the FAST exam, making it a poor tool to "rule-out." This is important as it urges physicians to not rely solely on a negative FAST exam when ruling out intra-abdominal injury but consider other factors including clinical gestalt, mechanism of injury, physical exam and laboratory work up.
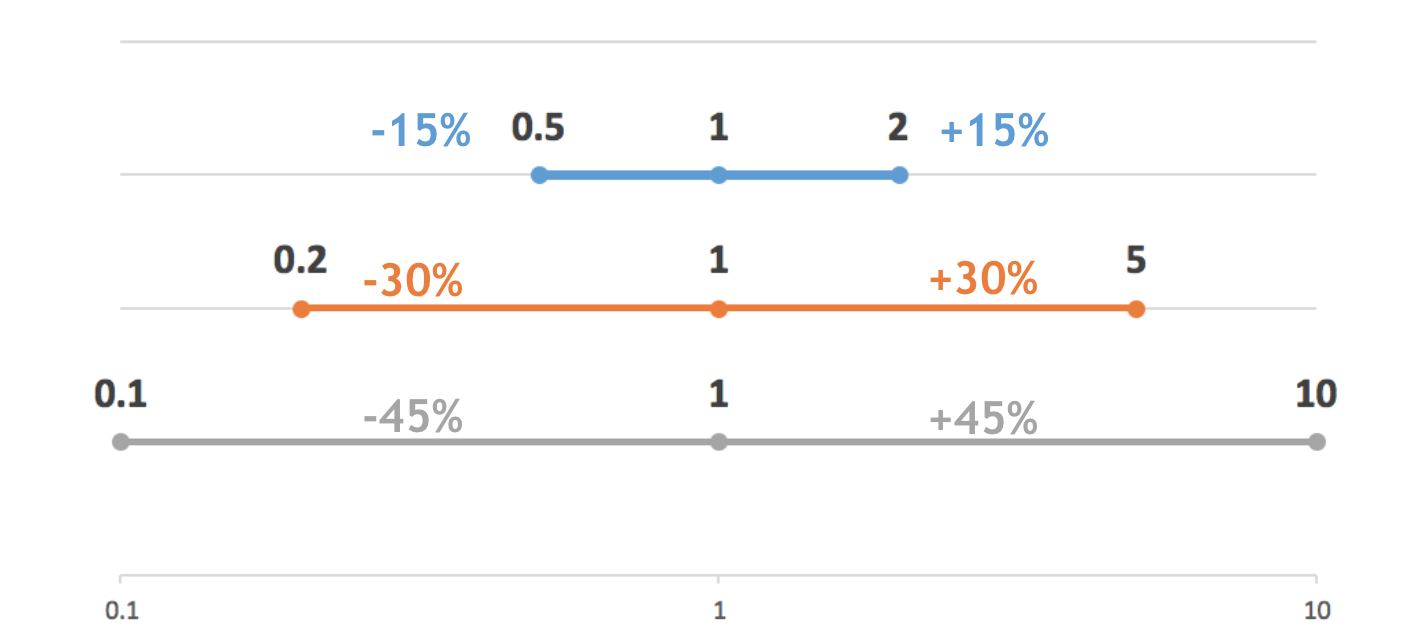
Additionally, to better understand the magnitude of this paper's findings it is important to known what a likelihood ratio really tells us. The following image is a quick way to think about likelihood ratios. A positive likelihood ratio of 2 should increase your probability of disease ( resulting in your post test probability) by 15%, 5 by 30% and 10 by 45%. Likewise a negative likelihood ratio of 0.5 should decrease your probability of disease by 15%, 0.2 by 30% and 0.1 by 45%.
The Bottom Line
Bedside ultrasonography is a highly specific diagnostic tool to rule in intra-abdominal injury following blunt trauma but should be used in conjunction with clinical gestalt, physical exam findings and laboratory values when ruling out injury.
Authors
This post was written by Olga Miakicheve, MS4 at UCSD. It was edited by Michael Macias, MD.
References
-
- Simel, D. (2012). Does This Adult Patient Have a Blunt Intra-abdominal Injury?. JAMA, 307(14), 1517. doi:10.1001/jama.2012.422